
BYLINE: Mary Gillam, Medical Editor, Point of Care
Overweight and obesity are states of excessive fat accumulation that present risks to health. With their increased prevalence over the last half century, obesity and its many complications have become a leading major public health problem. Obesity is typically diagnosed by calculation of the body mass index, which also can be used to classify the severity of obesity. Body mass index correlates moderately well with adiposity, although there is considerable variability in percentage body fat and presence of comorbidities and health risk factors on an individual level for a given BMI value(1).
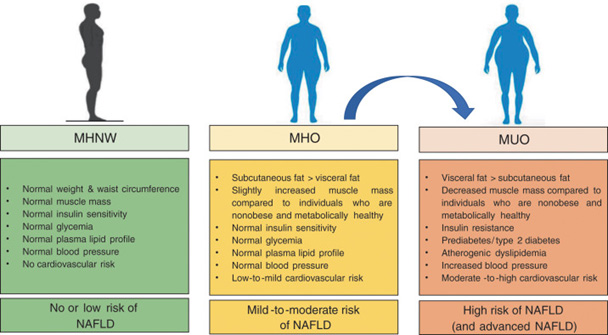
Obesity is often associated with a constellation of metabolic abnormalities, including hypertension, glucose intolerance, insulin resistance, dyslipidemia, nonalcoholic fatty liver disease, and the metabolic syndrome, which are important risk factors for type 2 diabetes and atherosclerotic cardiovascular disease. (see Figure 1)
Figure 1. Main cardiometabolic parameters among individuals with healthy normal weight versus metabolically healthy obesity and metabolically unhealthy obesity (8).
However, not all people with obesity have metabolic complications. Metabolically healthy obesity is a concept derived from clinical observations that a subgroup of people with obesity do not exhibit cardiometabolic abnormalities. The identification of this group came from analysis of data showing that this subgroup of obese individuals appear to have a lower risk of obesity-related cardiometabolic diseases than that which would be estimated from the positive association between body mass index and cardiometabolic risk (2). Based on such data, it was subsequently suggested, albeit controversially, that identifying such individuals would be useful since these patients may not require aggressive treatment as they were thought to be less likely to develop subsequent cardiometabolic complications (3). However, more recent data from long-term outcome studies demonstrate that a substantial proportion of metabolically healthy obese patients often convert to a metabolically unhealthy state, and do in fact develop cardiometabolic disease, including overt coronary artery disease itself 4–6. The finding that conversions from metabolically healthy to metabolically unhealthy obesity occur regularly suggests that metabolically healthy obesity represents a transient state, rather than a defined subgroup of obesity that remains stable.
The concept of metabolically healthy obesity developed from observations made decades ago that individuals with obesity have a different susceptibility to diabetes and atherosclerosis, which, in part, could be related to body fat distribution. At present, a set of universally accepted defining criteria for metabolically healthy obesity has not been established. Most experts agree that metabolically healthy obesity is typically marked by the absence of any metabolic and cardiovascular disease, including type 2 diabetes, dyslipidemia, hypertension, and atherosclerotic cardiovascular disease ASCVD in a person with obesity. One set of practical criteria for metabolically healthy obesity that has been proposed for adults includes (1) a diagnosis of obesity (BMI ≥30 kg/m2) AND (2) demonstration of the following: serum triglycerides ≤150 mg/dl), serum HDL-cholesterol concentrations >40 mg/dl (in men) or >50 mg/dl (in women), systolic blood pressure (SBP) ≤130 mmHg, diastolic blood pressure ≤85 mmHg, no antihypertensive drug treatment and no drug to lower serum glucose (7).
Additional physiologic traits of a metabolically healthy state include adequate cardiorespiratory fitness, preserved insulin secretion and sensitivity, and a predilection for lower body subcutaneous fat distribution (as opposed to liver or visceral fat) (8). (Figure 1)
Data on the prevalence of metabolically healthy obesity show a great range of variation and are confounded by the lack of standardized criteria for this phenotype. One recent meta-analysis that included 12 cohort and 7 intervention studies found that ~35% of the obese patients were considered metabolically healthy, though there were significant regional, ethnic, age, and sex differences and results were influenced by the criteria used to define metabolic health (9).
Metabolically healthy obesity is a transient phenotype which can convert into and from metabolically unhealthy obesity during cycles of weight loss and weight regain in response to obesity treatments and recidivism, respectively(10). Data from longitudinal studies indicate that ~30% to 50% of people with metabolically unhealthy obesity convert to a state of metabolically healthy obesity over the course of 4 to 20 years of follow-up (4,5). 30-year follow-up data from over 90,000 participants of the Nurses’ Health Study verified the frequent transition from metabolically healthy to metabolically unhealthy obesity and demonstrated a decline in metabolic health with age across the entire BMI range(6). These findings are corroborated by a meta-analysis of 12 studies including more than 5900 individuals with 3–10-year follow-up, which demonstrated that almost half of the participants classified with metabolically healthy obesity developed at least 1 metabolic abnormality(9).
The major factors associated with the conversion of metabolically healthy obesity to metabolically unhealthy obesity are a decline in insulin sensitivity and an increase in fasting blood glucose (11). The risk of transitioning from metabolically healthy obesity to metabolically unhealthy obesity is greater in those with a very high BMI, older age, presence of hepatic steatosis, higher number of abnormal metabolic criteria (especially values that are close to the upper limit of the normal range), a poor lifestyle index (a composite of diet composition, leisure time physical activity, and cigarette smoking), and weight gain during the observation period (5,12–14). Taken together, these longitudinal studies demonstrate that metabolic health among those who are obese is not a stable condition and is prone to deteriorate with aging and continued weight gain.
In general, the risks of type 2 diabetes, cardiovascular disease, and all-cause mortality are greatest in people with metabolically unhealthy obesity, followed by those with metabolically healthy obesity and least in those who are metabolically healthy and lean (5,11,15–18).
The risk of cardiovascular events (myocardial infarction, sudden cardiac death, heart failure, and peripheral vascular disease) is lower in people with metabolically healthy obesity than in those with metabolically unhealthy obesity, but is still higher than in people who are metabolically healthy and lean (16,17). A report from The Health Improvement Network study demonstrated that those with metabolically healthy obesity still had an increased risk of cardiovascular disease, particularly heart failure, and even coronary artery disease (16). Likewise, an analysis of participants of the Nurses´ Health Study found that metabolically healthy obese individuals who were able to maintain metabolic health over a long time still had a 57% higher risk of cardiovascular disease than those women with a stable normal body weight (6). In the same study it was shown that the risk of cardiovascular disease clearly increased in women who converted from metabolically healthy to metabolically unhealthy obesity compared to those with stable metabolically healthy obesity (6). Finally, a meta-analysis that pooled data from 18 prospective observational studies and included 585,000 participants followed over a median of 10 years found that the risk of cardiovascular events was about 50% greater in people with metabolically healthy obesity at baseline than in people who were metabolically healthy and lean (15).
Hence, the risk of developing cardiovascular events depends on whether the metabolic profile phenotype remains stable and healthy, or worsens and converts to metabolically unhealthy obesity and the risk is directly related to the number of metabolic abnormalities that develop from baseline (5,16).
The risk of developing type 2 diabetes is substantially elevated in obese individuals who are metabolically unhealthy; it is moderately high in individuals who are obese but metabolically healthy and relatively low in people who are metabolically healthy and lean. A meta-analysis of prospective cohort studies estimated that the risk of developing type 2 diabetes is 5- to 20-fold greater in obese people who are metabolically unhealthy compared to those who are healthy and lean, whereas those with metabolically healthy obesity have a 4-fold greater risk of developing type 2 diabetes compared to those who are healthy and lean 11. One cohort study that followed body weight and metabolic parameters among 34,000 young men over a 6-year time frame found that overweight and obese individuals who were metabolically healthy at baseline still had an increased risk of developing type 2 diabetes, as compared to healthy lean individuals (19). The summation of these studies demonstrates that over time, metabolically healthy obesity confers less risk for developing incident diabetes compared to obesity with metabolic dysfunction, but the long-term metabolic status still remains unfavorable.
In general, overweight and obesity are associated with an excess risk of all-cause mortality (20). Whether obese individuals who are metabolically fit are at increased risk for death is uncertain as the available data on risk of mortality is conflicting (15,18,21–23). There is some evidence that the risk of mortality is elevated for individuals with metabolically healthy obesity. One prospective cohort study that included over 10,000 individuals followed for 20 years found that those individuals who were obese but without any cardiometabolic abnormalities still had a 2-fold greater risk of mortality as compared to the reference group of healthy non-obese individuals (22). A systematic review and meta-analysis that combined data from eight cohorts and 61,000 patients found that metabolically healthy obese individuals had a higher rate of mortality compared with metabolically healthy normal-weight individuals (23). Notably, the mortality risk for those categorized as overweight did not achieve statistical significance, corroborating previous results that mortality risks fall along a continuum in proportion to body mass index (24).
Full Article
REFERENCES
1. Neeland IJ, Ross R, Després JP, et al. Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease: a position statement. Lancet Diabetes Endocrinol. 2019;7(9):715-725. doi:10.1016/S2213-8587(19)30084-1
2. Sims EAH. Are there persons who are obese, but metabolically healthy? Metabolism. 2001;50(12):1499-1504. doi:10.1053/meta.2001.27213
3. Stefan N, Häring HU, Schulze MB. Metabolically healthy obesity: the low-hanging fruit in obesity treatment? Lancet Diabetes Endocrinol. 2018;6(3):249-258. doi:10.1016/S2213-8587(17)30292-9
4. Echouffo-Tcheugui JB, Short MI, Xanthakis V, et al. Natural History of Obesity Subphenotypes: Dynamic Changes over Two Decades and Prognosis in the Framingham Heart Study. J Clin Endocrinol Metab. 2018;104(3):738-752. doi:10.1210/jc.2018-01321
5. Mongraw-Chaffin M, Foster MC, Anderson CAM, et al. Metabolically Healthy Obesity, Transition to Metabolic Syndrome, and Cardiovascular Risk. J Am Coll Cardiol. 2018;71(17):1857-1865. doi:10.1016/j.jacc.2018.02.055
6. Eckel N, Li Y, Kuxhaus O, Stefan N, Hu FB, Schulze MB. Transition from metabolic healthy to unhealthy phenotypes and association with cardiovascular disease risk across BMI categories in 90 257 women (the Nurses’ Health Study): 30 year follow-up from a prospective cohort study. Lancet Diabetes Endocrinol. 2018;6(9):714-724. doi:10.1016/S2213-8587(18)30137-2
7. Lavie CJ, Laddu D, Arena R, Ortega FB, Alpert MA, Kushner RF. Healthy Weight and Obesity Prevention: JACC Health Promotion Series. J Am Coll Cardiol. 2018;72(13):1506-1531. doi:10.1016/j.jacc.2018.08.1037
8. Lonardo A, Mantovani A, Lugari S, Targher G. Epidemiology and pathophysiology of the association between NAFLD and metabolically healthy or metabolically unhealthy obesity. Ann Hepatol. 2020;19(4):359-366. doi:10.1016/j.aohep.2020.03.001
9. Lin H, Zhang L, Zheng R, Zheng Y. The prevalence, metabolic risk and effects of lifestyle intervention for metabolically healthy obesity: A systematic review and meta-analysis. Med (United States). 2017;96(47). doi:10.1097/MD.0000000000008838
10. Appleton SL, Seaborn CJ, Visvanathan R, et al. Diabetes and cardiovascular disease outcomes in the metabolically healthy obese phenotype: A cohort study. Diabetes Care. 2013;36(8):2388-2394. doi:10.2337/dc12-1971
11. Bell JA, Hamer M, Batty GD, Singh-Manoux A, Sabia S, Kivimäki M. Incidence of metabolic risk factors among healthy obese adults: 20-year follow-up. J Am Coll Cardiol. 2015;66(7):871-873. doi:10.1016/j.jacc.2015.06.014
12. Guo F, Garvey WT. Cardiometabolic disease risk in metabolically healthy and unhealthy obesity: Stability of metabolic health status in adults. Obesity. 2016;24(2):516-525. doi:10.1002/oby.21344
13. Hashimoto Y, Hamaguchi M, Fukuda T, Ohbora A, Kojima T, Fukui M. Fatty liver as a risk factor for progression from metabolically healthy to metabolically abnormal in non-overweight individuals. Endocrine. 2017;57(1):89-97. doi:10.1007/s12020-017-1313-6
14. Espinosa De Ycaza AE, Donegan D, Jensen MD. Long-term metabolic risk for the metabolically healthy overweight/obese phenotype. Int J Obes. 2018;42(3):302-309. doi:10.1038/ijo.2017.233
15. Zheng R, Zhou D, Zhu Y. The long-term prognosis of cardiovascular disease and all-cause mortality for metabolically healthy obesity: A systematic review and meta-analysis. J Epidemiol Community Health. 2016;70(10):1024-1031. doi:10.1136/jech-2015-206948
16. Caleyachetty R, Thomas GN, Toulis KA, et al. Metabolically Healthy Obese and Incident Cardiovascular Disease Events Among 3.5 Million Men and Women. J Am Coll Cardiol. 2017;70(12):1429-1437. doi:10.1016/j.jacc.2017.07.763
17. Eckel N, Meidtner K, Kalle-Uhlmann T, Stefan N, Schulze MB. Metabolically healthy obesity and cardiovascular events: A systematic review and meta-analysis. Eur J Prev Cardiol. 2015;23(9):956-966. doi:10.1177/2047487315623884
18. Hamer M, Stamatakis E. Metabolically healthy obesity and risk of all-cause and cardiovascular disease mortality. J Clin Endocrinol Metab. 2012;97(7):2482-2488. doi:10.1210/jc.2011-3475
19. Twig G, Afek A, Derazne E, et al. Diabetes risk among overweight and obese metabolically healthy young adults. Diabetes Care. 2014;37(11):2989-2995. doi:10.2337/dc14-0869
20. Adams KF, Schatzkin A, Harris TB, et al. Overweight, Obesity, and Mortality in a Large Prospective Cohort of Persons 50 to 71 Years Old. N Engl J Med. 2006;355(8):763-778. doi:10.1056/nejmoa055643
21. Kuk JL, Rotondi M, Sui X, Blair SN, Ardern CI. Individuals with obesity but no other metabolic risk factors are not at significantly elevated all-cause mortality risk in men and women. Clin Obes. 2018;8(5):305-312. doi:10.1111/cob.12263
22. Johnson W, Bell JA, Robson E, Norris T, Kivimäki M, Hamer M. Do worse baseline risk factors explain the association of healthy obesity with increased mortality risk? Whitehall II Study. Int J Obes. 2019;43(8):1578-1589. doi:10.1038/s41366-018-0192-0
23. Kramer CK, Zinman B, Retnakaran R. Are metabolically healthy overweight and obesity benign conditions?: A systematic review and meta-analysis. Ann Intern Med. 2013;159(11):758-769. doi:10.7326/0003-4819-159-11-201312030-00008
24. Flegal KM, Kit BK, Orpana H, Graubard BI. Association of all-cause mortality with overweight and obesity using standard body mass index categories a systematic review and meta-analysis. JAMA - J Am Med Assoc. 2013;309(1):71-82. doi:10.1001/jama.2012.113905
25. Magkos F. Metabolically healthy obesity: What’s in a name? Am J Clin Nutr. 2019;110(3):533-537. doi:10.1093/ajcn/nqz133
Cookies are used by this site. To decline or learn more, visit our cookie notice.
Copyright © 2024 Elsevier, its licensors, and contributors. All rights are reserved, including those for text and data mining, AI training, and similar technologies.